

Clinical diagnosis
Case 74
【Progress】
He was advised to receive further respiratory examination such as bronchoalveolar lavage (BAL) in our hospital but he craved to return and consult with the physician in the local clinic.
【Discussion】
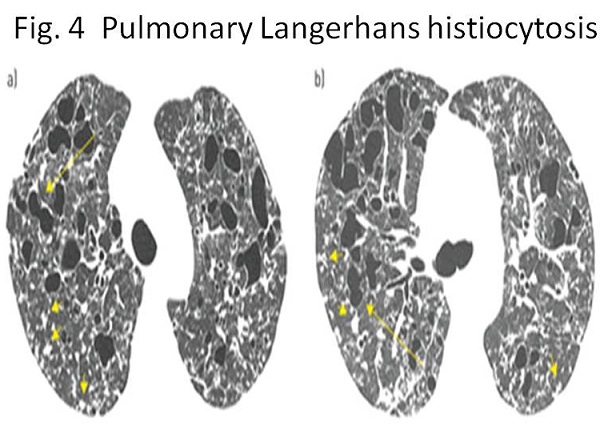
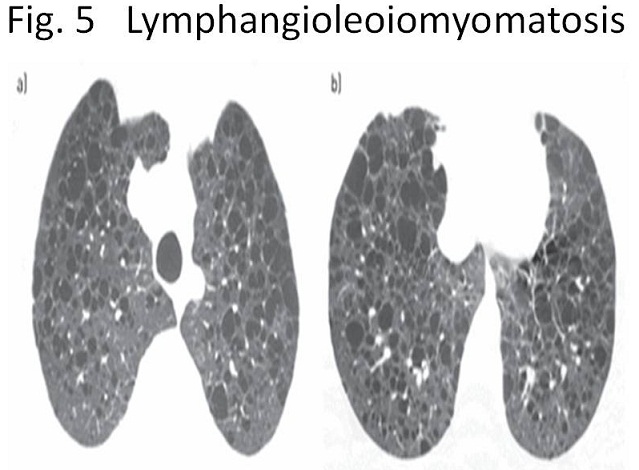
Lymphocytic interstitial pneumonia (LIP) is categorized in one of interstitial lung diseases based on pathological findings which revealed infiltration of T cells to broncho-vascular bundle (1). LIP is also one of polycystic lung diseases based on radiological findings (2). As representative polycystic diseases, LIP, pulmonary Langerhans cell histiocytosis (Fig. 4) and lymphangioleiomyomatosis (Fig. 5) are listed. CT images of these cystic diseases are different and specific in each. The difference must be attribute to the origin or mechanism of generating cysts. It is useful to recognize how these cysts are microscopically formed for making imaging diagnosis.
LIP is microscopically featured by diffuse infiltration of lymphocytes (predominant T cells), plasma cells and occasional histiocytes surrounding lymphatic channels at peri-broncho-vascular bundle, alveolar wall and subpleural areas (3, 4). There is no proof of an environmental allergen. Abundant peribronchial germinal centers exist and the airway lumen is often compressed. Cyst is formed by respiratory bronchiolar stenosis or occlusion due to peribronchiolar lymphoid infiltration, inducing air trapping and distal airway dilatation (1,3, 4). It indicates the size of cyst is almost as large as that of pulmonary lobule.
Pulmonary Langerhans cell histiocytosis is microscopically featured by Langerhans cells infiltration to peri-broncho-vascular bundle and formation of granulomas. These granulomas enlarge, inducing cavitation and occlusion of respiratory bronchioles, leading to respiratory bronchiole dilation and formation of cavities and cysts (5). These cysts might merge, forming bizarre forms (Fig. 4). Namely, the cyst pattern of pulmonary Langerhans cell histiocytosis represent the mixture of airway luminal dilatation and the cavity.
Lymphangioleiomyomatosis (LAM) is microscopically features by LAM cells infiltration to terminal bronchiole, inducing occlusion or severe stenosis of terminal bronchiole (6). As a result, it causes airway dilatation of terminal bronchioles, respiratory bronchioles and alveolus, resulting in accumulated cysts (Fig. 5).
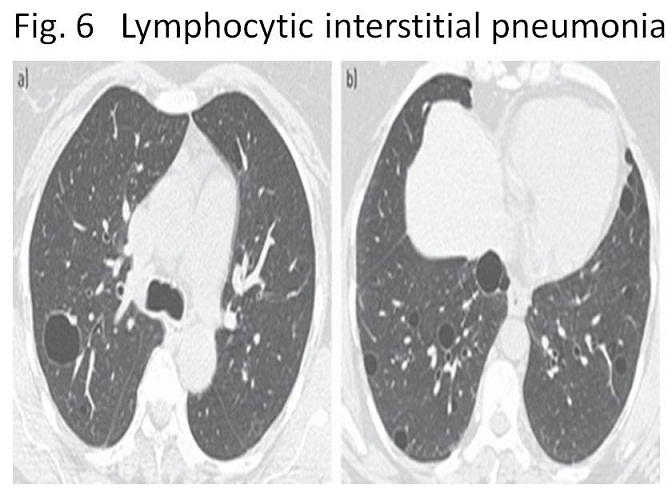
LIP is known to be one of autoimmune and lymphoproliferative disorders. Approximately one third of LIP is associated with Sjogren’s syndrome, AIDS and pulmonary drug reactions (1, 3, 4). LIP might be related to IgG4 disease or EBV infection and might lead to lymphoma, or might be spontaneous. The cysts are seen in up to 80% of the patients, typically not so many and less than 3 cm in size (Fig.6)(1, 3, 4). The clinical course of LIP is variable dependent on the presence or absence of basic disease. LIP is often stable without treatment and sometimes it improves spontaneously.
In our case, he got medicines for diabetes mellitus regularly which are not proven to be causative for LIP. He had no history of having immune disorder diseases. Then, his LIP is considered to occur spontaneously. Although histological examination was not attempted, chest CT showed a typical figure of LIP, localized round ground glass opacity and scattered several cysts sized less than 3 cm in both lobes (Figs 1-3).
【Summary】
We present a seventy three-year-old male with persistent cough and mild fever. Chest CT showed localized round ground glass opacity and scattered several cysts sized less than 3 cm in both lobes, indicating a typical image of Lymphocytic interstitial pneumonia (LIP). We should keep in mind that CT image of LIP composed of patchy ground glass opacity and scattered cysts of less 3 cm which are formed by infiltration of lymphocytes and plasma cells to broncho-vascular bundle and compressive stenosis and occlusion of respiratory bronchiole, inducing air trapping and airway dilatation.
【References】
1.Silva CI et al. Diffuse lung cysts in lymphoid interstitial pneumonia: high-resolution CT and pathologic findings. J Thorac Imaging. 2006 Aug;21(3):241-4.
2.Angelica F et al. Multiple cystic lung disease. European Respiratory Review 2015 24: 552-564; DOI: 10.1183/16000617.0046-2015
3.Ichikawa Y, et al. Lung cyst formation in lymphocytic interstitial pneumonia: CT features. J Comput Assist Tomogr 1994; 18: 745–748.
4.American Thoracic Society, European Respiratory Society. American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classification of the Idiopathic Interstitial Pneumonias. Am J Respir Crit Care Med 2002; 165: 277–304.
5.Abbott GF, et al. From the archives of the AFIP: pulmonary Langerhans cell histiocytosis. Radiographics 2004; 24: 821–841.
6.Juvet SC, Molecular pathogenesis of lymphangioleiomyomatosis: lessons learned from orphans. Am J Respir Cell Mol Biol 2007; 36: 398–408.
2017.10.4
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.