

Clinical diagnosis
Case 29


He admitted in our hospital to obtain drip infusion and antibiotics for several days. His medical condition was getting improved and discharged seven days later. He returned to his work with healthy condition.
【Discussion】
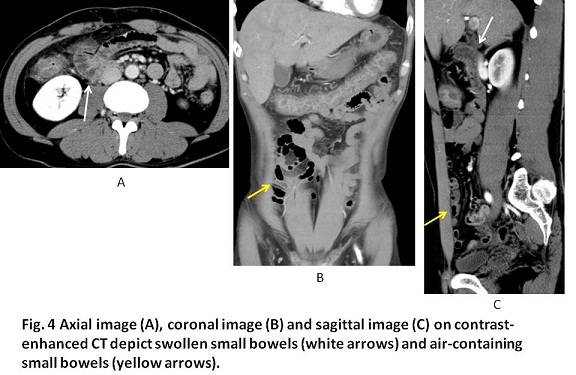
Campylobacter coli are gram-negative rods or spirals that produce an inflammatory, sometimes bloody, diarrhea and abdominal pain (1-5). The organism inhabits the intestinal tracts of a wide range of cattle such as chicken, pig and cow (1, 2). Contamination from raw meats or livers of the cattle leads to food-borne disease. Campylobacter infection can also be transmitted via water-borne outbreaks and direct contact with animals or animal products (1-5). Campylobacter account for up to 20% of acute bacillary diarrhea, but are often not detected at routine stool culture (1, 2). The main site of attack is the colon (4, 5). Campylobacter diarrhea is usually accompanied by fever and abdominal pain and causes watery diarrhea (1-5). Nausea, vomiting, headache, and myalgias may also be present, and tenesmus is a common feature (1-5). The majority of patients with Campylobacter diarrhea have some component of segmental colitis, usually beginning in the small bowel and progressing distally to the cecum (4, 5). In our case, symptoms of fever of 38 to 39 centigrade, abdominal pain, water diarrhea and tenesmus more than 10 times a day, little food ingestion were found. Further, CT showed almost entire colitis and enteritis.
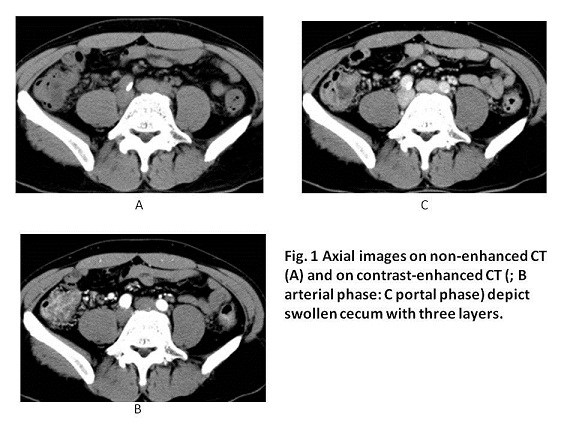
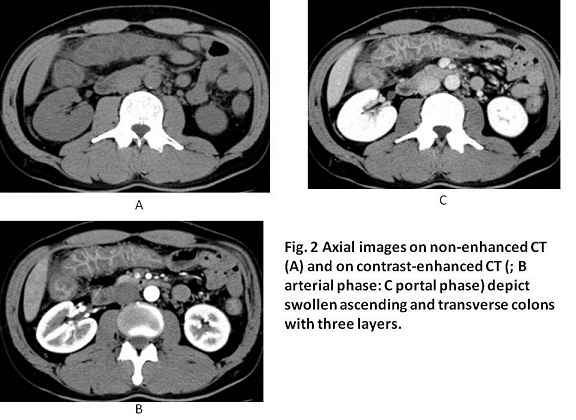
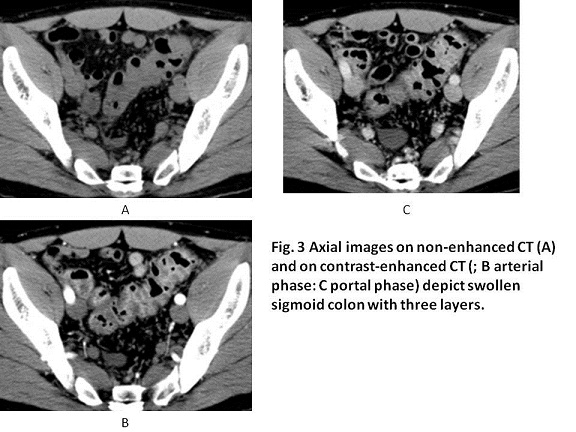
Escherichia coli (E Coli) O157 or O104, Salmonella, Campylobacter, Yersinia enterocolotics, Vibrio parahemolytics and Shigera are listed as the species of the common infectious colitis (6). One of the common CT findings of the infectious colitis is the mural thickening of ascending colon: a three-layer-structure which composed of mucosal layer, edematous submucosal layer and smooth muscle layer (6-8). In our case, contrast-enhanced CT showed well-enhanced mucosal layer and smooth muscle layer and ill-enhanced swollen submucosal layer, leading to the more prominent visualization of three layers than non-enhanced CT.
The CT findings of three-layer-structure of ascending colon in the patients with infectious colitis are non-specific (6-8) but specific characters of the infectious colitis are known. For examples, E coli O157 infection often induces peritonitis with the existence of dirty adipose tissue, ascitis and mesenteric swollen lymphnodes (9). Shiga toxin producing from E coli O104 affects the descending colon with upstream distension of the transverse/ascending colon and differs from other types of colitis (10, 11). Yersina entrocolotics often induces enlarged mesenteric lymphnodes and mural thickening in terminal ileum including appendix which should be differentiated from appendicitis (12, 13). Vibrio parahemolytics was found in 1950s by Fujino K in regional outbreak in Sennshu area situated at the south of Osaka by eating a contaminated tiny fish called Shirasu (14) . Vibrio parahemolytics species often inhabit in the warm sea water of summer and very weak in coldness (14). Although the incidence of Vibrio parahemolytics infection is getting less because of the development of cooling system, the swollen colitis and enteritis are found as non-specific colitis on abdominal CT (6).
【Summary】
We present a case with infectious colitis caused by Campylobacter whose symptoms were fever, abdominal pain and water diarrhea more than 10 times a day. Contrast-enhanced CT showed the marked colitis of the entire colon and enteritis that the mural wall of the colon composed of three-layer-structure of mucosal layer, edematous submucosal layer and smmoth muscle layer. Although symptoms and CT findings were non-specific, knowledge and recognition of the findings of other infectious colitis will help in patient evaluation and appropriate treatment.
【References】
1.Skirrow MB, Blaser MJ. Clinical aspects of Campylobacter infection. In: Campylobacter, 2nd ed, Nachamkin I, Blaser MJ (Eds), ASM Press, Washington DC 2000. p.6
2.Skirrow MB, Blaser MJ. Campylobacter jejuni. In: Infections of the gastrointestinal tract, 2nd ed, Blaser MJ, Smith PD, Ravdin JI, et al (Eds), Lippincott Williams and Wilkins, Philadelphia 2002. p.719.
3.Matsuaki S, Katyama A. Studies of food poisoning due to outbreaks of Campylobacter jejuni between 1980 and 1982 in Yamaguchi prefecture, Japan. Yamaguchi J Vet Med 1984; 11:53.
4.Tasaka K, et al. Invasive Campylobacter jejuni/coli Infections: 9 Case Reports at a Single Center between 2000 and 2015, and a Review of Literature Describing Japanese Patients Kansenshogaku Zasshi. 2016 May;90(3):297-304.[Article in Japanese]
5.Siegal D, et al. Campylobacter jejuni pancolitis mimicking idiopathic ulcerative colitis Heart Lung. 2005 Jul-Aug;34(4):288-90.
6.Horiki N, at al. CT evaluation of infectious colitis. Nihon Shokakibyo Gakkai Zasshi. 2002 Aug;99(8):925-34.[Article in Japanese]
7.Thoeni RF, Cello JP. CT imaging of colitis. Radiology. 2006;240 (3): 623-38.Radiology (full text) - doi:10.1148/radiol.2403050818 - Pubmed citation
8.Navaneethan U, et al. Infectious colitis. Curr Opin Gastroenterol. 2011 Jan;27:66-71. doi: 10.1097/MOG.0b013e3283400755.
9.Hiraka Tet al. Computed Tomographic Findings of Enterohemorrhagic Escherichia coli O157 Infection: An Analysis of a 7-Case Regional Outbreak. J Comput Assist Tomogr. 2015 May-Jun;39(3):406-8. doi: 10.1097/RCT.0000000000000209.
10.Bannas P et al. Shiga toxin-producing E. coli O104:H4 outbreak 2011 in Germany: radiological features of enterohemorrhagiccolitis. Rofo. 2013 May;185(5):434-9. doi: 10.1055/s-0032-1330520. Epub 2013 Feb 25
11.Matsunaga M, et al. CT images of enterohaemorrhagic Escherichia colicolitis. BMJ Case Reports 2016; doi:10.1136/bcr-2015-213548
12.Antonopoulos P et al. An emergency diagnostic dilemma: a case of Yersinia enterocolitica colitis mimicking acute appendicitis in a beta-thalassemia major patient: the role of CT and literature review. Emerg Radiol. 2008 Mar;15(2):123-6. Epub 2007 Jul 10.
13.Puylaert JB, et al. Mesenteric adenitis and acute terminal ileitis: US evaluation using graded compression. Radiology. 1986 Dec;161(3):691-5.
14.Takeda Y, et al. Vibrio parahemolytics 3rd edition Kinndai syuppann (in Japanese) 1990 ISBN 4874024750
2016.10.26
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.