

Clinical diagnosis
Case 22
We explained treatments for carotid aneurysm such as clipping and coil packing. Because she had no symptoms, it was difficult for her to decide the choice. She claimed to obtain the second opinion. She has not determined yet to undergo whether receiving surgical clipping, coil packing or watchful observation.
【Discussion】
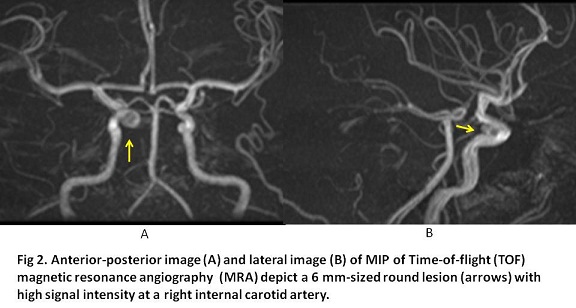
According to Fischer’s classification (1), a carotid artery is divided into 5 parts; C1 from bifurcation of anterior cerebral artery to branching of posterior communicating artery; C2 from branching of posterior communicating artery to branching of ophthalmic artery; C3 from branching of ophthalmic artery to exit of cavernous sinus; C4 surrounded by cavernous sinus; C5 from inlet of the cavernous sinus to outlet of carotid artery canal. In our case, the carotid artery aneurysm situated at the genu of U configuration of internal carotid artery corresponded to C3 as shown in Fig 2B.
Although the cause of carotid aneurysm is still unknown, it is considered that the stress to vascular wall by hypertension and anatomical branching site, and the fragility of vessel wall by smoking and gene predisposition, are relevant with the formation of carotid aneurysm. Vlak, et al. (2) reported using the meta-analysis that unruptured intracranial aneurysm was found with the incidence of 3.2 % of the adults of fifties or older, and the onset ratio was 6.9-fold in multiple polycystic kidney, 3.4-fold in the family history with cerebral aneurysm and 1.6-fold in women. Further, they clarified with case-control study that Odds ratio was 3.0 in smoking cohort, 2.9 in hypertension cohort and 8.3 in smoking + hypertension cohort (2). In our case, she had no habit of smoking and her blood pressure was within normal limits but had the family history of her elder sister having a rupture of cranial aneurysm.
As main treatments of cerebral aneurysm, surgical clipping and endovascular coil packing are listed. In these days, the number of endovascular treatment is increasing accompanied with its progress and prevalence and the less incidence of adverse effect compared to surgical treatment. The incidence of complete shrinkage after coil packing varies 54% to 91% (3, 4). Meanwhile, in 10 years and 20 years after surgical clipping, the incidence of the subarachnoid hemorrhage is reported to be 1.4 % and 12.4%, respectively (5). The choice of treatments for carotid aneurysm is still controversial.
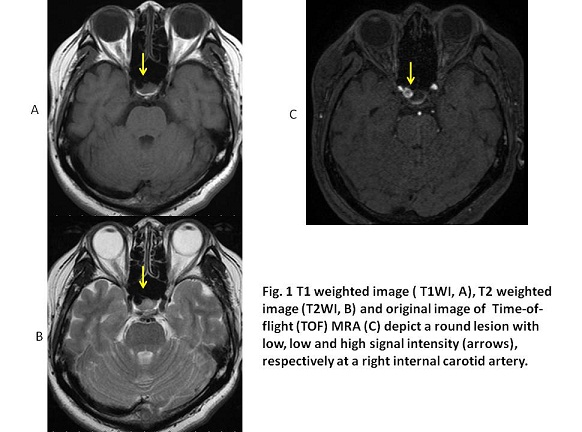
Time-of-flight (TOF) MRA is used for non-contrast bright-blood of neurovascular system (6). Repeated RF pulses in short time, cause least signal intensities of normal tissue surrounding vessels because time is too short for hydrogen nucleus to return from magnetic saturated state to unsaturated state. Meanwhile, unsaturated-flowing blood flows constantly in the vessel, which induces high signal intensity. TOFMRA is the method to visualize the inflow new unsaturated blood as high signal intensities (6). High speed imaging of gradient echo method with the minimum time of echo (TE < 7 msec) is actually used for TOFMRA. In addition, a pre-saturation pulse is usually applied above each slice in order to disappear signal from traversing veins (6). A maximum intensity projection (MIP) rendering technique is then used to create the MR angiogram. Three-dimensional (TOF) MR angiography using multi slab method was used in this case.
【Summary】
We present a forty one-year-old female whose MR angiography using (TOF) MR angiography depicts a cerebral aneurysm with the size of 6 mm at C3 of the right internal carotid artery. She had no episode of smoking and hypertension but a family history that her elder sister who is two years older died of the rupture of the internal carotid aneurysm. Although she hesitated to receive the treatment, she is being under the inspection using MRI&MRA of 6 months follow-up for future treatment.
【References】
1.Fischer E. Die Lageabweichungen der vorderen Himaterie im Gefassbild. Zentralbl Neurochir 1938;3:300-313
2.Vlak MH, et al. Prevalence of unruptured intracranial aneurysm, with emphasis on sex, age, comorbidity, country, and time period: a systemic review and meta-analysis. Lancet Neurol 2011; 10: 626-636
3.Murayama Y et al. Guglielmi detachable coil embolization of cerebral aneurysms: 11 years’ experience. J Neurosurg 2003; 98:959-966
4.Brilstra EH, et al. Treatment of intracranial aneurysms by embolization with coils: a systematic review. Stroke 1999; 30: 470-476
5.Tsutsumi K, et al. Risk of subarachnoid hemorrhage after surgical treatment of unruptured cerebral aneurysm. Stroke 1999; 30: 1181-1184
6.Saloner D. An introduction to MR angiography. Radiographics 1995;15:453-465
2016.9.7
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.