

Clinical diagnosis
Case 14
The patient received anti-convulsive agent and steroid therapy that brought about the relief of the facial convulsion, inducing to enable to continue the speech rehabilitation.
【Discussion】
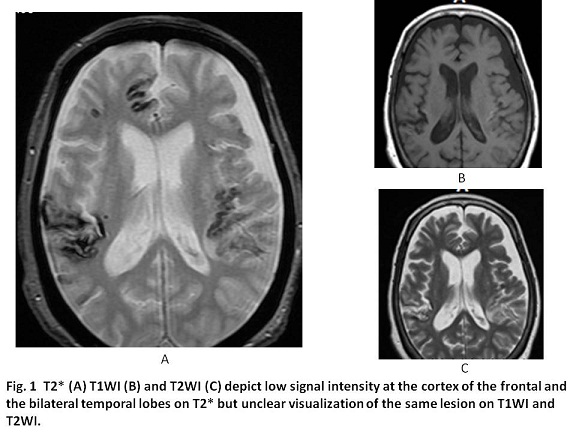
Cerebral amyloid angiopathy (CAA) is known as a form of angiopathy in which amyloid deposits in the walls of small arteries of the cerebral cortex and lepto-meninges. It might cause cerebral cortical hemorrhage and/or subarachnoid hemorrhage. In autopsied studies, the incidence of CAA is increased accompanied with aging: 5-9% of the age of sixties: up to 43-58% in over the age of 90 (1-3). CAA can be found on screening of MRI using T2* in up to 16% of asymptomatic elderly patients in the previous report (1-3). Symptomatic CAA is usually presented with an intracranial hemorrhage and/or inflammatory reaction called CAA-related inflammation (1, 2). As manifests of CAA, the various symptoms of higher brain dysfunction are listed (1). In our case, cognition impairment, speaking disturbance, convulsion and right hand weakness were found.
As the premortem diagnosis of CAA, the Boston criteria stated that multiple hemorrhage restricted to lobar, cortical or subcortical lesions on the basis on CT or MRI, age of more than 55, and the absence of other causes of hemorrhage. Small hemorrhages caused by hypertension are usually seen in basal ganglion. In the previous reports, MR examinations do not always include T2* gradient-echo sequences that enables recognition of microbleeds (1-3). Our case meet this criteria and T2* depicts the multiple cortical and subcortical hemorrkhages.
T2WI are obtained following a 90 degree RF pulse and a 180 degree RF pulse. A 180 degree RF pulse is used for eliminating the main magnetic field inhomogeneity and the differences in magnetic susceptibility among various tissues (4, 5). Then, T2WI indicates the image obtained by the signal of pure spin-spin interaction. Meanwhile, T2* weighted images are obtained a 90 degree RF alone omitting a procedure of a 180 degree RF pulse (5). As a result, T2* weighted images are obtained by the signals of spin-spin interaction and magnetic susceptibility among various tissues (5). Then, T2* weighted images are used to depict hemorrhage, calcification, and iron deposition in various tissues and lesions (4, 5).
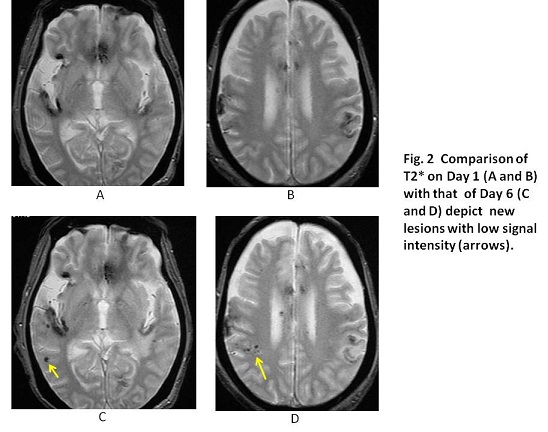
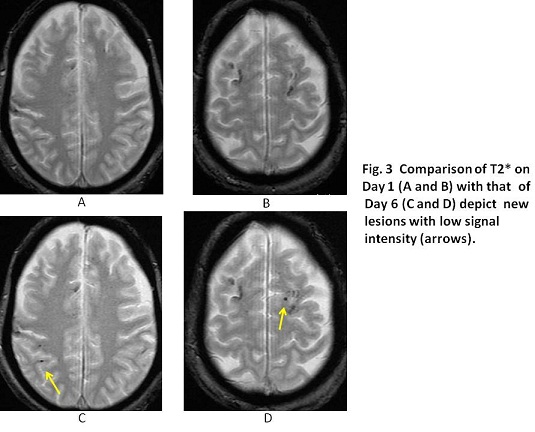
Deoxyhemoglobin existing in veins and hemosiderin in old breeds are paramagnetic molecules whereas oxyhaemoglobin in arteries is diamagnetic (4, 5). The presence of deoxyhaemoglobin and hemosiderin causes a susceptibility difference between the vessel and its surrounding tissue, leading to a reduction in the value of T2* but not the presence of oxyhemoglobin (5). In our case, compared with T2*WI on Day 1, T2*WI on Day 7 depict several new low signal intensities which indicate new hemorrhage including deoxyhemoglobin and the unchanged low signal intensities which indicate original hemorrhage including hemosiderin. T2*WI might be available to use for showing the new hemorrhage.
【Summary】
A seventy three-year-old female suffering from cognition decline and speech disturbance was admitted in our hospital for speech rehabilitation. T2*WI on Day 1 depicted multiple lesions at the cortex with low signal intensities. Day 7, her worsening speaking ability, right hand tremor, handwriting disability and convulsion with intermittent facial paralysis were newly found. T2*WI on the same day depicted new several low signal intensities at the cortex. T2*WI was useful to detect the new hemorrhage of cerebral amyloid angiopathy in our case.
【References】
1.Sakaguchi,H, et al. Cerebral amyloid angiopathy-related inflammation presenting with steroid-responsive higher brain dysfunction: case report and review of the literature. J Neuroinflammation 2011; 8: 116
2.Savoiardo M, et al. Case 159: Cerebral Amyloid Angiopathy–related Inflammation. Radiology; 2010; 256
3.Castro A, et al. Cerebral Amyloid Angiopathy Associated with Inflammation: Report of 3 Cases and Systematic Review. J Stroke Cerebrovasc Dis 2015; 24 2039-2048
4.FInstP PJAOBEPFIPSM, CSci JWMFIPEM. Farr's physics for medical imaging. Saunders Ltd. (2007) ISBN:0702028444
5.Stark DD, Bradley WG, Bradley WG. Magnetic resonance imaging. C.V. Mosby. (1999) ISBN:0815185189.
2016.7.13
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.